Section Branding
Header Content
More kids are dying of drug overdoses. Could pediatricians do more to help?
Primary Content
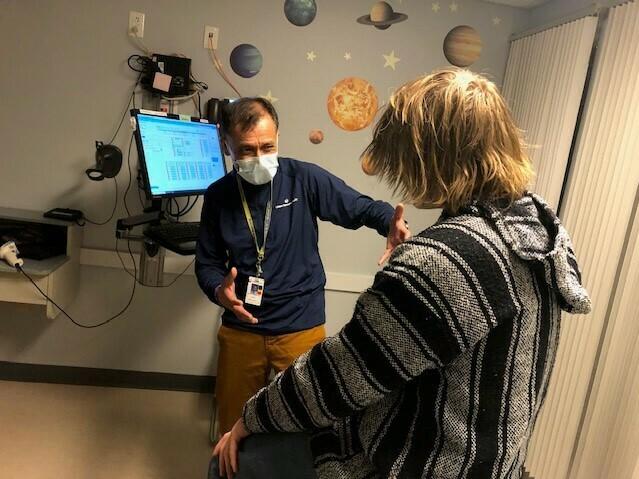
A 17-year-old boy with shaggy blond hair steps onto the scale at Tri-River Family Health Center in Uxbridge, Massachusetts.
After he's weighed, he heads for an exam room decorated with decals of planets and cartoon characters. A nurse checks his blood pressure. A pediatrician asks about school, home life and his friendships.
This looks like a routine teen check-up, the kind that happens in thousands of pediatric practices across the U.S. every day – until the doctor pops this question.
"Any cravings for opioids at all?" asks Dr. Safdar Medina. The patient shakes his head, no.
"None, not at all?" Medina says again, to confirm.
"None," says the boy named Sam, in a quiet but confident voice.
We're only using Sam's first name because he could face discrimination in housing and job searches based on his prior drug use.
Medina is treating Sam for an addiction to opioids. He's prescribed a medication called buprenorphine. It curbs cravings for the more dangerous and addictive opioid pills. Sam's urine tests don't show any signs of the Percocet or Oxycontin pills he was buying on Snapchat, the pills that fueled Sam's addiction.
"What makes me really proud of you, Sam, is how committed you are to getting better," says Medina, whose practice is part of UMass Memorial Health.
Are pediatricians an untapped resource to fight addiction?
The American Academy of Pediatrics recommends offering buprenorphine to teens addicted to opioids. But only 6% of pediatricians do, according to survey results.
In fact, buprenorphine prescriptions for adolescents were declining as overdose deaths for 10-19-year-olds more than doubled. These overdoses, combined with accidental opioid poisonings among young children, have become the third leading cause of death for U.S. children.
"We're really far from where we need to be and we're far on a couple of different fronts," says Dr. Scott Hadland, chief of adolescent medicine at Mass General for Children, and co-author of the study that surveyed pediatricians about addiction treatment.
That survey showed that many pediatricians don't think they have the right training or personnel for this type of care — although Medina and other pediatricians who do manage patients with an addiction say they haven't had to hire any additional staff.
Some pediatricians responded to the survey by saying they don't have enough patients to justify learning about this type of care, or don't think it's a pediatrician's job.
"A lot of that has to do with training," says Dr. Deepa Camenga, Associate Director for Pediatric Programs, Yale Program in Addiction Medicine.
"It's seen as something that's a very specialized area of medicine and therefore people are not exposed to it during routine medical training."
Camenga and Hadland say medical schools and pediatric residency programs are adding information to their curricula about substance use disorders, including how to discuss drug and alcohol use with children and teens.
But the curricula aren't changing fast enough to help the number of young people struggling with an addiction, not to mention those dying after taking just one pill.
In an ironic but deadly development, drug use among adolescents has actually declined – but drug-associated deaths are up.
The main culprits are fake Xanax, Adderall or Percocet pills laced with the powerful opioid fentanyl. Nearly 25 percent of recent overdose deaths among 10-to-19-year-olds were traced to counterfeit pills.
"Fentanyl and counterfeit pills is really complicating our efforts to stop these overdoses," says Dr. Andrew Terranella, the CDC's expert on adolescent addiction medicine and overdose prevention. "Many times these kids are overdosing without any awareness of what they're taking."
Terranella says pediatricians can help by stepping up screening for — and having conversations about — all types of drug use.
He also suggests pediatricians prescribe more naloxone, the nasal spray that can reverse an overdose. It's available over the counter, but Terranella, who practices in Tucson, Arizona, says a prescription may carry more weight with patients.
Trying out different prescription methods
Back in the exam room, Sam is about to get his first shot of Sublocade, an injection form of buprenorphine that lasts 30 days. Sam's switching to the shots because he didn't like the taste of Suboxone, oral strips of buprenorphine that he was supposed to dissolve under his tongue. He was spitting them out before he got a full dose.
Many doctors also prefer the shots because patients don't have to remember to take them every day. But the injection is painful. Sam is surprised when he learns that it will be injected into his belly and will take 20-30 seconds.
"Is it almost done?" Sam asks, while a nurse coaches him to breathe deeply. When it's over, the staff joke out loud that even adults usually swear when they get the shot. Sam says he didn't know that was allowed. He's mostly worried about any residual soreness that might interfere with his evening plans.
"Do you think I can snowboard tonight?" Sam asks Dr. Medina.
"I totally think you can snowboard tonight," Dr. Medina says reassuringly.
Sam is going with a new buddy. Making new friends and cutting ties with his former social circle of teens who use drugs has been one of the hardest things, Sam says, since he entered rehab 15 months ago.
"Surrounding yourself with the right people is definitely a big thing you want to focus on," Sam said. "That would be my biggest piece of advice."
Buprenorphine wasn't offered earlier
For Sam, finding addiction treatment in a medical office jammed with puzzles, toys and picture books is not as odd as he thought it would be.
He's come to this appointment with his mom, Julie. She says she's grateful the family found a doctor who understands teens and substance use.
Before coming here, Sam had seven months of residential and outpatient treatment — without ever being offered buprenorphine to help control cravings and prevent relapse. Only 1 in 4 residential programs for youth offer it. When Sam's cravings for opioids returned, a counselor suggested Julie call Dr. Medina.
"Oh my gosh, I would have been having Sam here, like, two or three years ago," Julie says. "Would it have changed the path, I don't know, but it would have been a more appropriate level of care for him."
Some parents and pediatricians worry about starting a teenager on buprenorphine, which can produce side effects including long-term dependence. Pediatricians who prescribe the medication weigh the possible side effects against the threat of a fentanyl overdose.
"In this era, where young people are dying at truly unprecedented rates of opioid overdose, it's really critical that we save lives," says Hadland, chief of adolescent medicine at Mass General for Children. "And we know that buprenorphine is a medication that saves lives."
Addiction care can take a lot of time for a pediatrician. Sam and Dr. Medina text several times a week. Medina stresses that any exchange that Sam asks to be kept confidential is not shared.
Medina says treating a substance use disorder is one of the most rewarding things he does.
"If we can take care of it," he says, "We have produced an adult that will no longer have a lifetime of these challenges to worry about."
This story comes from NPR's health reporting partnership with WBUR and KFF Health News.
Bottom Content
