Section Branding
Header Content
Older adults are often misdiagnosed. Specialized ERs and trained clinicians can help
Primary Content

Errors in diagnosis are relatively common among older people. The reasons are many: older adults may have multiple conditions, take many medications, and illnesses can look very different in older people than they do in younger ones. Older adults may show different symptoms or none at all. And sometimes health care workers assume that whatever is bothering the patient is “because of your age.” All this can lead to older patients being either under-treated or over-treated.
Sometimes there are even worse outcomes. According to a recent study by researchers from Johns Hopkins University, almost 800,000 Americans die or are permanently disabled each year because of diagnostic errors.
But as the population of older adults expands rapidly, more attention is being paid to how to successfully treat them.
A special design
At Glen Cove Hospital on Long Island, a third of the people who arrive in the ER are over the age of 65.
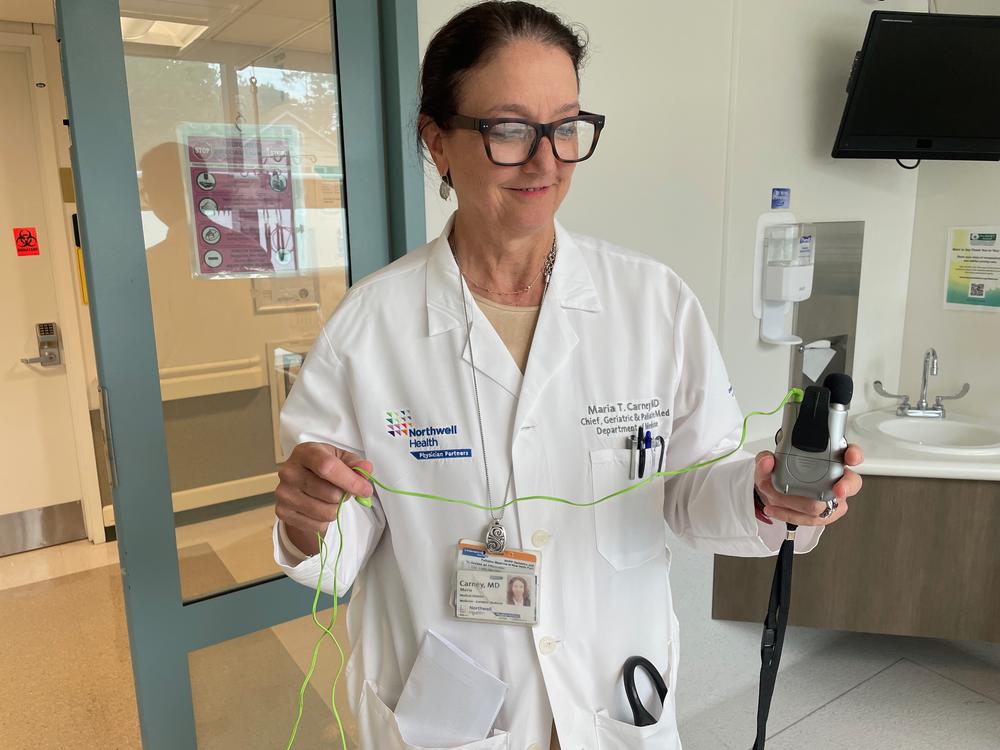
Dr Maria Carney is chief of geriatrics and palliative medicine for Northwell Health, the network that includes Glen Cove Hospital. She says an older person coming in may be weak or confused, and it could be their first time here.
“If you don’t know the person’s baseline,” she says, “if you don’t know there’s new medication started, if you don’t know that they had a fall a week ago and you can’t get that information because they’re not able to communicate, it’s very hard to diagnose accurately.”

But this emergency department is specially designed to accommodate older adults. Since late 2021, it has been accredited as a geriatric emergency department by the American College of Emergency Physicians. It’s one of more than 500 hospitals around the country that now has this designation.
What that means in practice is that you’ll find plenty of subtle enhancements for safety and comfort that you wouldn’t find in a regular ER.
For one thing, instead of cubicles with noisily drawn curtains — which can carry infection — the patient has a room of their own with a door, and glass that fogs up for privacy at the flick of a switch.
The floors are textured to make them less slippery, and instead of harsh, fluorescent light blaring from above, there is ambient lighting and plenty of daylight coming in through the windows.
“Oftentimes when you’re inside a hospital you don’t know what time of day it is and that can contribute to delirium,” says Carney. “So you’re trying to prevent delirium,” which can be a problem in older patients.

There are also tools to help with communication. Carney says when older patients arrive they may not have their eyeglasses or hearing aids with them, if they use them. She picks up an assisted hearing device, which looks like a tiny tape recorder with earphones plugged into it. Any patient who needs hearing help can use the earphones while the doctor or nurse speaks into the mic. The patient’s room is large, with plenty of room for medical staff to move around, and comfortable chairs for family members.
Carney says all this turns the emergency department into an easier place for older patients to be. With less stress and better communication, an accurate diagnosis is more likely.
More training needed
At UConn Health in Farmington, Conn., Dr. Patrick Coll, medical director for senior health, says there would be fewer diagnostic errors if more young doctors became geriatricians like him and Carney.
This year, he says, “There were just over 170 geriatric fellows placed in geriatric fellowship programs across the United States. There were more than a thousand cardiology fellowship positions filled.”
Cardiology, of course, is vital, too. But with the population of older people growing fast - especially those over 85 — Coll says the US needs more expertise in older bodies and minds.
“If we were training providers right across the board to better care for older adults, then I think we would get better care for older adults,” he says. “And I believe that the appropriate diagnosis would be a part of that spectrum of better care.”
Involve nurses
Nurses spend more time with older patients than anyone else, says Allie Tran, a nurse with a Ph.D who is a senior research scientist at MedStar Health Research Institute. She’s working on a project to involve nurses in improving diagnosis.
“Because what we’ve found when we’ve talked to nurses is many nurses don’t consider expressing a diagnosis as part of their scope or role,” she says. “You know, they say ‘that’s kind of the physician’s job.’”
She says ideally nurse, physician, patient and family members could work together on figuring out what’s wrong. She says sometimes a patient will only mention a particular point when the doctor has left the room, thinking it isn’t important. She says nurses can be the bridge between patient and physician, and make a real difference in the diagnosis.
Advocating for herself
As it is now, patients like Karla Stromberger, who is 80, say they have to be their own advocates at the doctor’s when a diagnosis feels off.
“To try and convince that person that something else is going on and to please listen, is just exhausting,” she says.
Stromberger, a retired physical therapist, had polio in the 1950s. As she’s aged she’s had a lot of health problems related to that. But, she says, too often medical staff don’t take her polio into account when they assess her, and many see her age before her symptoms.
“And they kind of go, ‘Well, OK, that’s an elderly patient’ — and we are elderly,” she says. “But some of us are competent enough, still, to be able to help them figure out what’s going on.”
When she can do that, she considers it a victory.
Bottom Content
