Section Branding
Header Content
'1619 Project' journalist lays bare why Black Americans 'live sicker and die quicker'
Primary Content
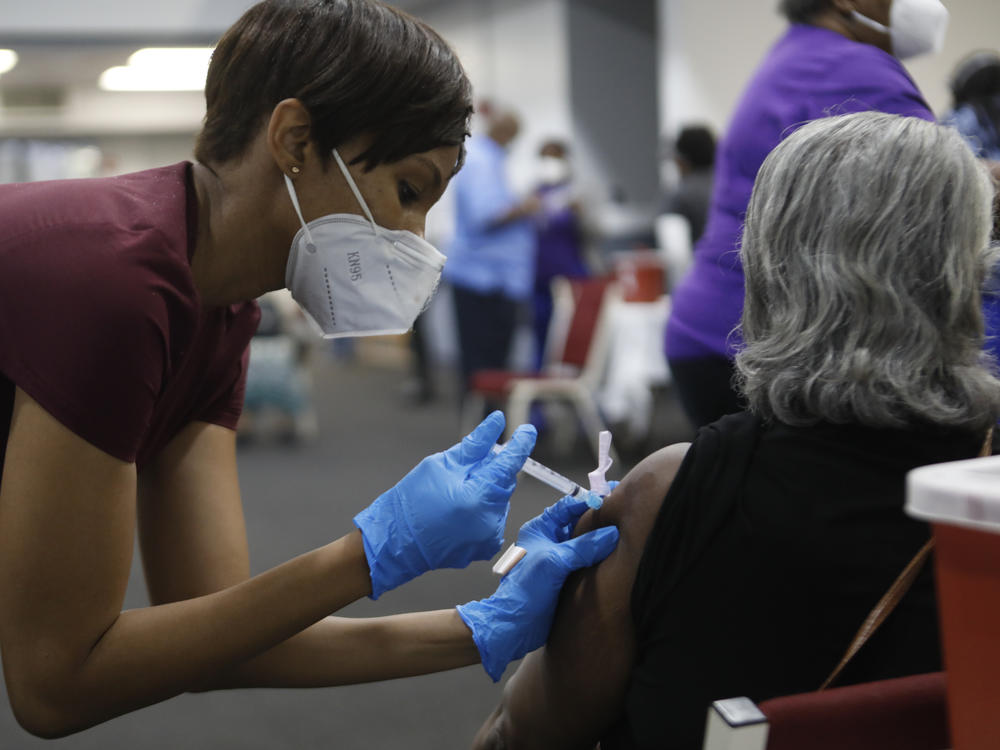
The COVID-19 pandemic laid bare the racial inequities that plague American health care, with Black people dying of the disease at a rate more than double that of white people.
Author Linda Villarosa has been writing about the racial disparities in health outcomes for decades and recently covered the topic for the New York Times' 1619 Project. She says that while she used to think poverty was to blame for Black Americans' health problems, she's now convinced that bias in the health care system and the "weathering" affect of living in a racist society are taking a serious toll on African Americans.
Villarosa points to "weathering" -- a concept developed by public health professor Dr. Arline Geronimus — as the wear on the body that results from prolonged exposure to stress: "Your heart rate goes up, your cortisol stress levels go up in your body. Your blood pressure rises," she says. "It's not good for the body. But when people are treated badly, that's what happens."
In her book, Under the Skin, Villarosa argues that any effort to close the gap in health outcomes must also address the structural racism that underpins the U.S. health care system. She points to historical myths about Black bodies — including the fallacy that Black people have a higher pain tolerance than white people — that continue to impact the way care is delivered.
In 2019, for instance, researchers from UNC-Chapel Hill published a study that showed that Black women did not receive as much pain management following a C-section as white women, even when everything else was the same — perhaps, Villarosa says, because of implicit biases among medical students and residents.
"That is alarming because those are the future doctors of America. And so that means that we need to do things differently here," she says.
Villarosa says that while she used to tiptoe around the word "racism" when she spoke on panels, she no longer feels like the need to avoid the term.
"We're not accusing individuals of being racist, but we're saying there is something wrong with what is happening in America," she says. "When you identify the problem, when you discuss the problem, it's easier to address the problem and come up with solutions than it is when you're pretending like it doesn't exist."
The following interview has been edited for length and clarity.
Interview highlights
On writing about the health crisis in Black America for Essence in the '80s, and assuming problems were "our own fault"
It was clear that there were racial health disparities. Black Americans had higher rates of so-called "lifestyle diseases," is what we called them then, and it was heart disease, diabetes, stroke, asthma. We knew that, but we just didn't understand the cause. And so the explanation was it's our own fault. So either it was something about our genetic makeup that was making us more sick, and also [causing] lower life expectancy and higher rates of infant mortality, or it was something we were doing wrong. So at Essence, the idea was, we can fix racial health inequality by just getting all the people [who read] our magazine, because those are the people we had access to, to just do better. And what we said is, if you know better, you do better.
On how Dr. Harold Freedman's research changed the way she understood racial disparities in healthcare
He looked at the health of men in Harlem and compared them to men in the impoverished country of Bangladesh. And it turned out that Black men in Harlem lived fewer years than men in Bangladesh. It was shocking. It was in the New England Journal of Medicine. So he came to speak to my class at the Harvard School of Public Health, my fellowship class, and I was so interested in everything he had to say. I was insisting to him that this is a problem of poverty. And one thing he said to me was, "Wait a minute, look at the population of Harlem. The population of Harlem isn't all impoverished. So if you are thinking that the problems of Black people, the health problems of Black people in America are only because of poverty, you're making a mistake and you're thinking is going to be wrong." What I learned from him is if you're looking at the problem through the wrong lens, you're coming up with incorrect and ineffective solutions.
On the myth that Black bodies feel less pain than white bodies
That myth started during the years of enslavement, and it was pushed by doctors and scientists at the time who also had a hand in keeping slavery intact. So the idea that if Black people had extreme tolerance to pain, you could hurt our bodies, you could beat us, whip us, take our children away and work us from sunset to sundown and it wouldn't matter.
What I learned was that myth was pushed using evidence in data in medical journals. So then fast forward, for me, to 2016 and it was a study out of the University of Virginia that looked at myths and mythology that [white] medical students still believed ... including the idea that Black people have a different kind of pain tolerance.
Other myths were that Black skin is thicker than white skin. Certainly that is a myth. Skin comes in all degrees of thickness. But if you believe that, it sort of speaks to a kind of a false invulnerability that Black people have that would allow us not have our pain treated in the same way.
On the myth that Black people have weaker lungs – and how there's a race correction to this day
There was a myth that, again, started during the years of slavery that Black people had inferior lung function. So it was sort of the opposite of the pain tolerance, one where we had a superpower and this was an inferiority. The idea was that because of these weak lungs, it was good for us to work in the fields because it was like a form of exercise, free labor as exercise. And this was a myth that was believed by doctors and again, pushed forward in medical journals, at medical conferences.
Fast forward to today and there's a machine called a spirometer that measures lung function, and often in these same machines that are used today, there's a race correction that assumes that Black people have inferior lung function. And I was thinking about this not long ago. A couple of years ago, I had a lung-function test because I was getting over bronchitis. And then I started thinking, I wonder if I got the race correction, which would have been really unfair because I was raised in Denver, which is the Mile High City, so I have really good lungs. So it's incorrect to assume a racial inferiority without looking at other ways that I might be different, including having been raised in the Mile High City.
On maternal death rates being higher among Black women in the U.S.
I heard this while I was playing soccer on a weekend from a woman who was an international lawyer. She was telling me, "Did you know that the United States is the only country where the number of women who die or almost die in childbirth is going up?" So I said, "Oh, no, I didn't know that." Then she said, "It's driven by Black women because Black women are 3 to 4 times more likely to die or almost die." I was still under the impression, even in 2017, that this was an issue of poverty. So I was arguing with her and then she stopped me cold because she said, "Education is not protective." If you're a Black woman with a master's degree or more, you are still more likely to die or almost die than a white woman with an eighth grade education. So that struck me.
It also struck me that I had had a low birth-weight baby, which was really unusual for someone in that I was so healthy. I was working as the health editor of Essence magazine. I was a public figure as a healthy person trying to do everything right. And then I had this low birth-weight baby. I've heard so many other stories from other Black women, including Serena Williams, who had a difficult birth. ... This is just so widespread. And it's I think that my article struck a chord for people who had been experiencing this but never heard it discussed.
On how "weathering" affects other groups of people
I decided to go to West Virginia, to an area that was having an HIV outbreak. It was having an HIV outbreak because of opioids. So West Virginia, as we know, was flooded with opioid pills. And then they were pulled back from the streets. So people got addicted to heroin, so they started using heroin and sharing needles. So that created an HIV outbreak. So I was just curious to see what happens [when] you treat people badly, you inundate them with pills, and then you yank them away and then they get addicted to heroin. Then they're blamed for their condition with less interrogation of what actually happened, what pharmaceutical companies did.
What I found was, right away, the first thing I noticed was people looked so much older than I thought. I was always mis-guessing everyone's age. I saw people that were homeless. There was such an extreme amount of shame from the people. There was so much pain. And I just thought, this is weathering, too. When people get treated badly, they blame themselves. They don't get treatment and care. They get ridicule and a lack of support. This is what happens to you, your body ages. So it's really anyone who's mistreated and marginalized.
On how studying the mistreatment of Black people's health can help other people too
Because our experience has lasted so long in America, our mistreatment began in 1619, and it goes up until today, so we're the ones who have been the most well-studied. We are the ones whose bodies were commodified, which meant that there was close attention paid to our health and our well-being, but also our pain and damage. And so it's interesting to look at Black bodies and it's important, but discrimination and harm hurts anyone.
Sam Briger and Joel Wolfram produced and edited this interview for broadcast. Bridget Bentz, Molly Seavy-Nesper and Laurel Dalrymple adapted it for the web.
Copyright 2022 Fresh Air. To see more, visit Fresh Air.
Bottom Content
