Section Branding
Header Content
The top White House monkeypox doc takes stock of the outbreak — and what's next
Primary Content
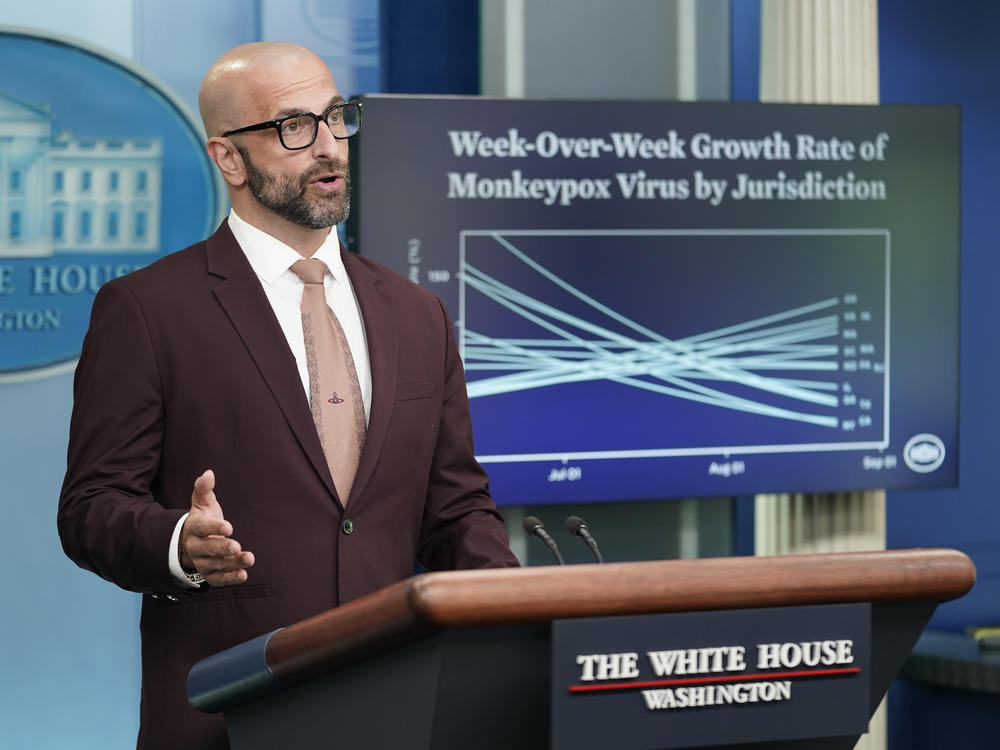
The U.S. monkeypox outbreak appears to be slowing.
New infections are starting to decline in some large cities where the virus hit early and spread quickly. And while there's still uncertainty, the Centers for Disease Control and Prevention is currently projecting that the outbreak "will most likely continue to grow very slowly" over the next few weeks.
Health officials say it's cause for cautious optimism – but not complacency.
Much of the improvement is being attributed to temporary changes in sexual behavior, and progress is uneven, with new cases rising in some parts of the U.S. and disproportionately affecting certain minority populations, such as Black and Latino men.
The U.S. is relying on a strategy of vaccinating high-risk populations – largely gay and queer people, particularly men who have sex with men in social networks where the virus is spreading. But there are still open questions: scientists don't yet have much real-world data on how well the JYNNEOS vaccine – approved by the Food and Drug Administration in 2019 – stops infection and transmission. And the vaccination campaign must be successful at reaching those who could most benefit from the shots.
NPR caught up with Dr. Demetre Daskalakis, one month into his job as deputy coordinator for the White House Monkeypox Response, to talk about where the outbreak is headed, and what it's like to go from being an HIV doctor and queer health activist to being the out-and-proud face of the government's monkeypox response.
This conversation has been edited for length and clarity.
Pien Huang: As you look out over the next few weeks or months, where do you see the outbreak headed? Is it realistic to think we could get to virtually no cases in the U.S.?
Demetre Daskalakis: I think we're going to get to a point where we'll see occasional cases because of introductions [of the virus] from other places. We'll also potentially see small clusters. But in terms of this big ol' curve that we've been seeing, I think that's going to dissipate so it's no longer an outbreak, but more episodic.
If you look at the epidemiology of cases that happen outside of gay, bisexual and other men who have sex with men, there are a lot of terminal chains: you have somebody [with monkeypox], and then maybe their household contacts [get it] and then it ends.
I wouldn't be surprised if we continue to see little chains [of transmission]. Then, the vaccine would be used more for contact-focused vaccination as opposed to the population-based, behavior-based vaccination campaign [we have now].
You and other experts have credited changes in behavior for helping to slow the spread of monkeypox in the U.S. What does that mean for controlling the outbreak going forward, given that the virus has been spreading "almost exclusively" through sexual contact?
It is not impossible that we could see cases increase if behaviors regress. We definitely see that the messaging – from CDC and the U.S. government as well as interpretations by others – has really moved the needle, in terms of some of the behaviors associated with monkeypox exposure.
Single partnerships [meaning one-time sexual encounters] that men who have sex with men report are down – 50% have stopped doing them or reduced them – less anonymous sex, all of the things we advise as temporary measures, until we get vaccines into people's arms and they can go back to life as usual.
We're in this phase where getting the supply and maintaining the demand [for vaccines] is so important. It's reasonable to think people will change behavior for awhile, but not reasonable to think that they're going to change it forever. And we're not asking for forever, we're asking for now.
Why not frame this as a sexually transmitted infection? After all, gay and queer communities are generally pretty accustomed to talking about sexual health.
The jury's out on what this is going to be called. I think what's important is: monkeypox is sexually associated, no matter what.
What's important to me is less the semantics and more that we're giving the right advice, and that the places that people go [to seek information and care] are resourced to do the work.
A paper you co-authored that was posted recently shows that many monkeypox cases are being found in people with HIV and also those with a recent history of STIs. Why is this the case?
It's the social network, and the behaviors that are associated with it, that may imply why HIV-positive men who have sex with men are overrepresented.
One of my favorite lines in the paper actually says – I like it so much, I'm going to read it to you verbatim – "It is important that systems for delivering HIV and STI care and prevention be leveraged for monkeypox evaluation, vaccination and other prevention interventions, and treatment."
[On Wednesday], sort of timed with this [paper], CDC released updated guidance to some of its grantees that said that they could use both staffing and funds that are earmarked for HIV and STDs to actually support monkeypox.
It's kind of groundbreaking. It puts it into this context of this thing called a syndemic, which is like the different epidemics that interact. So it weaves monkeypox into where it belongs, which is together with the work that we do every day to prevent HIV and STIs.
Recent CDC data show that vaccination rates may be declining. It seems like we're nearing a point where many of the people who want to get vaccinated have done so. How do you make sure people get the two shots even if cases are going down?
So first, supply, supply, supply – supply is important because some of the demand changes are driven by the idea that, "There's no vaccine, so why should I look for it?"
We've addressed this with the new intradermal vaccine strategy increasing supply on the ground and with [getting] more [vials], whether it's from the company overseas, or with onshore fill-and-finish of the vaccine.
We've [sent vaccine doses to] some large events that signal "the doctor is open" and vaccines are more accessible.
The other work that we're doing is around equity. We [recently sent doses to] Atlanta Black Pride, where they did almost 4,000 vaccines, also with Southern Decadence in New Orleans, where they did about 3,500. Those are the big versions.
But we'll also soon be releasing a pathway to small equity interventions that are for niche, more innovative ideas that reach deeper into the community.
Is there a danger that people are looking at the current numbers and saying "monkeypox is slowing, so I don't need a vaccine?"
Always, there's a risk of people saying, "Oh look, the curve is down and we're going to move on." But we've been really good about messaging that two vaccines plus two weeks means that you have optimal coverage. So the experience I'm hearing so far is that people are interested in getting their two shots and they just want [health authorities] to open up availability [so they can] get them.
What's it been like for you to be in such a visible role as the gay/queer person that's the face of the White House monkeypox response?
My very first hour of doing this, I got to meet with the President and he said my job is to make sure that we're really working hard for the LGBTQ community, especially in the vein of equity. So literally, I landed and was told to do exactly what I love doing. It's been great.
I get to work with Bob Fenton, [the White House Monkeypox Response Coordinator], who is like a rock star from the perspective of large event emergencies. I'm learning some really valuable things from him that are definitely outside my normal wheelhouse.
Is there any tension between the role you have as a government official versus your longtime work as an HIV doctor and gay health advocate?
There's being the doctor for one person at a time and then there's being a doctor for an entire community and our entire population. There's a very specific responsibility you have when you're making decisions for millions of people. I value [my time working with patients]. I feel like those experiences with individual humans and patients end up making all of this make sense to me.
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Bottom Content
